
Doctors are controlling scalpel-wielding robots in real operations from afar, finds Rose Eveleth. Is this the future of surgery?
When Mehran Anvari picks up a surgical instrument and cuts into somebody’s flesh, he doesn’t use his own hands. In fact, he’s not even in the room. He operates on patients that are 400 kilometres away.
From a console in St Joseph’s Hospital in Hamilton, Canada, he controls a robot surgeon in an entirely different part of the country, slicing, stitching and removing bits of the body. He’s carried out more than 20 operations so far, including colon operations and hernia repairs.
The technology behind long-distance surgery is now mature enough to be used more widely, allowing people to access world-leading expertise and better healthcare without having to travel. Could it become the norm in hospitals?
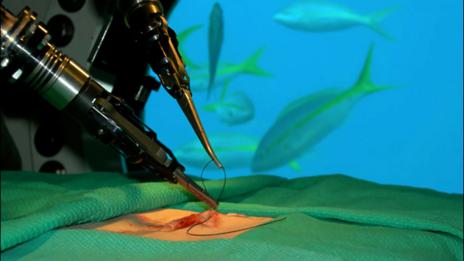
A robot simulates stitches on an underwater base, while being controlled by surgeon Mehran Anvari from the surface
The birth of telesurgery didn’t happen with everyday procedures in mind. In fact, it was issues away from Earth that got the robotic doctor movement going. As soon as people began to truly consider human spaceflight, they started to wonder how they might treat a human thousands of miles away from any doctor.
In the 1970s, Nasa suggested that researchers look into the option of remote-controlled robots to operate on astronauts. Since then, Nasa and the US Army have worked steadily to create reliable robots that could operate on somebody at a distance. In 2006, Anvari used a robot to sew up a cut on someone living in the ocean, at the Aquarius underwater base, to simulate what space telesurgery might be like.

The remote-controlled Da Vinci robot surgeon performs heart surgery
But, as with most things that begin with space and the military, the innovations of telesurgery research have also been bleeding into civilian life. In 2001, the first transatlantic operation was conducted by surgeons in New York on a patient in France. And in recent years, the first market-ready robotic surgeon called the da Vinci system has been introduced, usually controlled by a surgeon nearby.
Anvari’s robot, called Zeus, works in a community hospital that lacks the same facilities and expertise as his own. But other than the location, he says not much is different. “It’s the same as if I were sitting in the operating room,” he says. “I have both my hands on the robot the same way I would have instruments in both hands.”
He move the robotic camera that serves as his eyes, and can speak with the nurses in the operating room with the patient to give them instructions. “Basically, it’s the same as if I were next to the patient, just using telecommunication and robotics. It doesn’t feel different.”

Mehran Anvari controls his robot surgeon, conducting a keyhole surgery (St Joseph’s Healthcare)
Better landlines and hard-wired internet connections have made lag less of an issue. When Anvari operated on his first set of patients, there was a delay of about 175 milliseconds which is imperceptible.
Yet with distance comes more lag time, and interruptions still risk disaster. “It’s not realistic to expect these robots to go into autopilot mode and finish the surgery,” says Tamas Heidegger, a researcher at Obuda University in Budapest who studies space telesurgery.
This will certainly be an issue for operations conducted at great distances – such as in deep space or Mars. Out there, robots that use algorithms and databases to make decisions during surgery will be required, says Mangai Prabakar, an engineer at Florida International University who designs smart robots.
“If they can just maintain the communication link between Earth and the space shuttle, then they can be guided by the surgeon on earth,” she says. “But Mars is really far, and we can’t communicate over such a huge distance.” Mangai says that for long distance space travel, we’re going to have to build robots that we can trust to do full surgeries without a human guiding the scalpel on Earth. And that will require incredibly powerful computers.
After all, surgery is hard. “You can have a master surgical plan, and things can go wrong,” says Haidegger. “We can’t predict what’s going to happen in an advanced stage of surgery. If blood circulation collapses, breathing stops, or there’s an unforeseen reaction to drugs or chemicals, these are cases that you need a trained surgeon on site.”

A surgeon controls the Da Vinci robot surgeon, viewing a 3D image of the body (SPL)
Nonetheless, Haidegger believes a remote-control robot augmented with artificial intelligence will come with time and increased demand. And that demand will likely come from space as much as Earth. The growth of commercial spaceflight has generated interesting questions about telerobotic surgeries.
Given that people of various ages and health backgrounds can fly with SpaceX and Virgin Galactic, the probability of someone needing emergency surgery on a commercial flight could be higher, and the demand for telesurgeons higher with it.
In the meantime, more and more doctors on Earth are showing signs of embracing the general idea of telemedicine to treat and diagnose patients. And by 2025, the US Department of Defense wants to have a Trauma Pod that would allow surgeons to perform operations on soldiers from a distance.
So will future operations be done by somebody in another hospital, or even another country or planet? “The science is already there,” Anvari says, “the other stuff is what’s holding us back.”
Those issues include ethical problems and regulations. In principle, the technology could spark a new wave of medical tourism. Patients unable to afford healthcare in the US, for instance, could turn to surgeons in other countries. Yet if something goes wrong, who should be considered liable – those in the robot-operating theatre or the surgeon working from Cuba?
Perhaps the most important issue, however, is whether patients will be comfortable with a surgeon they have never met face-to-face. Would you let a surgeon remove your kidney or repair your heart from hundreds of kilometres away? You may soon be asked the question.
Culled from The BBC
Follow Us